 Sabadell rejects the merger with BBVA and will fight to remain alone
Sabadell rejects the merger with BBVA and will fight to remain alone In Germany, the far left wants to cap the price of “doner kebabs”
In Germany, the far left wants to cap the price of “doner kebabs” Israel-Hamas war: Gaza between hope of truce and fear of Israeli offensive in the South
Israel-Hamas war: Gaza between hope of truce and fear of Israeli offensive in the South “Mom, Dad, please don’t die”: in the United States, a nine-year-old child saves the lives of his parents injured in a tornado
“Mom, Dad, please don’t die”: in the United States, a nine-year-old child saves the lives of his parents injured in a tornado The presence of blood in the urine, a warning sign of bladder cancer
The presence of blood in the urine, a warning sign of bladder cancer A baby whose mother smoked during pregnancy will age more quickly
A baby whose mother smoked during pregnancy will age more quickly The euro zone economy grows in April at its best pace in almost a year but inflationary pressure increases
The euro zone economy grows in April at its best pace in almost a year but inflationary pressure increases Children born thanks to PMA do not have more cancers than others
Children born thanks to PMA do not have more cancers than others “House of the Dragon”, “Succession”… Max, the new streaming platform from HBO and Discovery, launched in France on June 11
“House of the Dragon”, “Succession”… Max, the new streaming platform from HBO and Discovery, launched in France on June 11 The A13 motorway will finally reopen this Friday, in one direction only
The A13 motorway will finally reopen this Friday, in one direction only TNT commission of inquiry: tensions between LFI deputies and Macronists before the vote on the report
TNT commission of inquiry: tensions between LFI deputies and Macronists before the vote on the report Apple unveils a new, more efficient iPad range
Apple unveils a new, more efficient iPad range The Gaza War invites itself to the 2024 Pulitzer Prizes
The Gaza War invites itself to the 2024 Pulitzer Prizes Judith Godrèche presents a short film on sexual violence in Cannes
Judith Godrèche presents a short film on sexual violence in Cannes Kevin Spacey: new trial in sight in London for the American actor, for sexual assault
Kevin Spacey: new trial in sight in London for the American actor, for sexual assault Taylor Swift fans make London pub Black Dog their new place of pilgrimage
Taylor Swift fans make London pub Black Dog their new place of pilgrimage Omoda 7, another Chinese car that could be manufactured in Spain
Omoda 7, another Chinese car that could be manufactured in Spain BYD chooses CA Auto Bank as financial partner in Spain
BYD chooses CA Auto Bank as financial partner in Spain Tesla and Baidu sign key agreement to boost development of autonomous driving
Tesla and Baidu sign key agreement to boost development of autonomous driving Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV
Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV The home mortgage firm rises 3.8% in February and the average interest moderates to 3.33%
The home mortgage firm rises 3.8% in February and the average interest moderates to 3.33%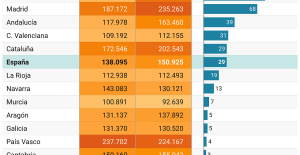 This is how housing prices have changed in Spain in the last decade
This is how housing prices have changed in Spain in the last decade The home mortgage firm drops 10% in January and interest soars to 3.46%
The home mortgage firm drops 10% in January and interest soars to 3.46% The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella
The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella Institutions: senators want to restore the accumulation of mandates and put an end to the automatic presence of ex-presidents on the Constitutional Council
Institutions: senators want to restore the accumulation of mandates and put an end to the automatic presence of ex-presidents on the Constitutional Council Europeans: David Lisnard expresses his “essential and vital” support for François-Xavier Bellamy
Europeans: David Lisnard expresses his “essential and vital” support for François-Xavier Bellamy Facing Jordan Bardella, the popularity match turns to Gabriel Attal’s advantage
Facing Jordan Bardella, the popularity match turns to Gabriel Attal’s advantage Europeans: a senior official on the National Rally list
Europeans: a senior official on the National Rally list These French cities that will boycott the World Cup in Qatar
These French cities that will boycott the World Cup in Qatar “The future is for us”: “disappointed” and “proud” at the same time, Al-Khelaïfi sees the glass half full after the elimination of PSG
“The future is for us”: “disappointed” and “proud” at the same time, Al-Khelaïfi sees the glass half full after the elimination of PSG PSG: “Since January, these have not been my best matches,” agrees Zaire-Emery, who promises to “come back stronger”
PSG: “Since January, these have not been my best matches,” agrees Zaire-Emery, who promises to “come back stronger” “What is this question, honestly?” : Nasser Al-Khelaïfi (very) annoyed after PSG-Dortmund
“What is this question, honestly?” : Nasser Al-Khelaïfi (very) annoyed after PSG-Dortmund “I am the guy who has to score the goals”: Mbappé does not hide and assumes responsibility after PSG’s exit
“I am the guy who has to score the goals”: Mbappé does not hide and assumes responsibility after PSG’s exit
Dr Mathias Wargon is head of the Smur emergency department at Delafontaine hospital (Saint-Denis) and president of the Île-de-France regional observatory for unscheduled care.
No one is satisfied with the way the emergency department works anymore. Neither the patients, nor their loved ones, nor the caregivers in the emergency room or elsewhere. Should we give up?
Emergency rooms are a high-risk place. A lot of decisions are made quickly, with little information, and for several potentially serious patients treated simultaneously. The staff, who have a high turnover rate, are often young and inexperienced. Spot interruptions are common. A patient may be cared for by several successive teams with a possible loss of information, all leading to a lack of communication with families whose presence in the emergency room is considered an additional burden.
On the problem of overload, everything has been said. The increase in emergency room attendance is staggering: each year, 500,000 additional patients go there, reaching 22 million in 2019. And it continues. By the time it takes to build a service, it is already too small. This has consequences, described in the scientific literature: delays in care, excess mortality among the elderly, medical errors, lack of communication with patients, blackout for families, zero attractiveness and staff fleeing.
Also read: The emergency crisis, the most visible sign of a system that has become obsolete
One of the pitfalls frequently put forward is that of the emergency department (the departments where patients who are unable to return home are hospitalized). Despite the development of outpatient hospitalization (when the patient does not spend the night in hospital), competition between hospitalizations scheduled by services and those requested by emergencies remains keen. And the places in what we call downstream (returning home with help, follow-up care, and EHPADs) are too few, stranding many patients in hospital.
Let's say it right away: these problems are real and undeniable. But these are not the only explanations for the difficulties of emergencies, even if they are the easiest and allow us to blame all the dysfunctions on policies or ministries. But we cannot fail to talk about the responsibility of hospitals and emergency services themselves, requiring an examination of conscience that is not always pleasant.
Emergencies have changed, and the profession of emergency physician has become a medical specialty in its own right. We could hope that this would improve the situation of practitioners and their enthusiasm to work there. But the pre-eminence, in representative bodies, of doctors who still think that maintaining a good quality of life requires working part-time in the SAMU has not helped. And do we know that the national hospital emergency council has been chaired since its creation in 2009 by a professor of medicine who has never worked in the emergency room, and was renewed in this position a few months ago despite his imminent departure retired ? What message are we sending to staff?
Also read “Decongest” emergency services by the end of 2024: why the objective set by Macron seems difficult to achieve
Among the solutions, the regulation of emergencies seems to be unanimous, since it allows only patients whose condition requires the care for which they were designed to be sent there. We still need to be able to offer alternatives everywhere to patients who do not need the technicality of emergencies, but who need to see a doctor quickly. But above all, what should we think of services that barricade themselves and put a security guard at the entrance, preventing any contact with the nursing staff? And why ? This says a lot about the deterioration of relations between the population and these personnel, and the need to have coordinators or mediators.
Politicians and health officials are talking about the concept of “bed manager”. But it is often just a new name slapped on old and ineffective practices, a secretary or a nursing manager going around the hospital begging for beds. The real bed manager depends on management and imposes services on patients, even when they are reluctant. It is no coincidence that elderly people spend nights on stretchers: polypathological, complex to care for, they are rejected in favor of patients who we know will leave the hospital more quickly.
The emergency service is open 24 hours a day, seven days a week, now with continuous activity even in the deepest hours of the night. The hospital operates on office hours. It is becoming inevitable that waiting times for a radiological examination or a specialist's opinion will lengthen, contributing to the increase in the treatment time for all the patients present.
Also read: Preventable diseases, redundant actions: these ways to improve health
The internal organization of emergencies is often obsolete, dating from a time when the service willingly carried out what others did not do. This good Samaritan charge kills these services and is sometimes not financially recognized, which would nevertheless make it possible to expand the teams. Monitoring patients hospitalized but without a bed, or placed in pseudo-observation units while they are in intensive care, is a significant burden which is often not compensated in terms of staff, since it is unofficial. But if emergency doctors don't take care of it, no one will.
Insufficient staffing? In reality, even when there are enough staff, there is a shortage. Emergency practice requires continuing education and regular training. Training times are largely insufficient. How can we ensure optimal care for a very wide number of pathologies if we do not review frequently? Writing protocols that no one will ever read is only a good indicator for those who believe that quality is achieved from files.
Also read “Every year it’s worse”: emergencies under high tension this summer
In reality, before talking about the organization of the hospital and the health system, it is necessary to reorganize emergencies. We cannot continue in this complex system without a conductor. And yet, we have moved away from the classic managerial system. The local management, which is solely responsible for nurses and care assistants, is overwhelmed by tasks and meetings that distance it from staff. The department head often performs this function for a small part of his working time. However, emergencies are like a business. But what would we think of a boss who sometimes employs more than 100 people, has hundreds of customers every day, and who manages the business only when he has nothing else to do (here, see patients)?
Examples of services that work better than others (or less poorly if one is pessimistic) exist. The errors are known, some solutions too. We can no longer be satisfied with fatalism or injunctions. We cannot continue to carry out audits in emergency services when situations are catastrophic, without really implementing the solutions adopted. Does this have to happen through external action? Probably, when it is not possible to reform internally and what guides the functioning of the emergency room and the hospital is the balance of power between those in charge, rather than the interests of the patients.


















