 United States: divided on the question of presidential immunity, the Supreme Court offers respite to Trump
United States: divided on the question of presidential immunity, the Supreme Court offers respite to Trump Maurizio Molinari: “the Scurati affair, a European injury”
Maurizio Molinari: “the Scurati affair, a European injury” Hamas-Israel war: US begins construction of pier in Gaza
Hamas-Israel war: US begins construction of pier in Gaza Israel prepares to attack Rafah
Israel prepares to attack Rafah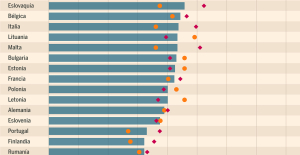 Spain is the country in the European Union with the most overqualified workers for their jobs
Spain is the country in the European Union with the most overqualified workers for their jobs Parvovirus alert, the “fifth disease” of children which has already caused the death of five babies in 2024
Parvovirus alert, the “fifth disease” of children which has already caused the death of five babies in 2024 Colorectal cancer: what to watch out for in those under 50
Colorectal cancer: what to watch out for in those under 50 H5N1 virus: traces detected in pasteurized milk in the United States
H5N1 virus: traces detected in pasteurized milk in the United States Private clinics announce a strike with “total suspension” of their activities, including emergencies, from June 3 to 5
Private clinics announce a strike with “total suspension” of their activities, including emergencies, from June 3 to 5 The Lagardère group wants to accentuate “synergies” with Vivendi, its new owner
The Lagardère group wants to accentuate “synergies” with Vivendi, its new owner The iconic tennis video game “Top Spin” returns after 13 years of absence
The iconic tennis video game “Top Spin” returns after 13 years of absence Three Stellantis automobile factories shut down due to supplier strike
Three Stellantis automobile factories shut down due to supplier strike A pre-Roman necropolis discovered in Italy during archaeological excavations
A pre-Roman necropolis discovered in Italy during archaeological excavations Searches in Guadeloupe for an investigation into the memorial dedicated to the history of slavery
Searches in Guadeloupe for an investigation into the memorial dedicated to the history of slavery Aya Nakamura in Olympic form a few hours before the Flames ceremony
Aya Nakamura in Olympic form a few hours before the Flames ceremony Psychiatrist Raphaël Gaillard elected to the French Academy
Psychiatrist Raphaël Gaillard elected to the French Academy Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV
Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV Tesla launches a new Model Y with 600 km of autonomy at a "more accessible price"
Tesla launches a new Model Y with 600 km of autonomy at a "more accessible price" The 10 best-selling cars in March 2024 in Spain: sales fall due to Easter
The 10 best-selling cars in March 2024 in Spain: sales fall due to Easter A private jet company buys more than 100 flying cars
A private jet company buys more than 100 flying cars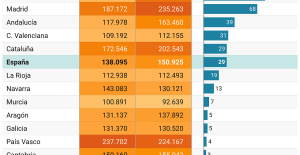 This is how housing prices have changed in Spain in the last decade
This is how housing prices have changed in Spain in the last decade The home mortgage firm drops 10% in January and interest soars to 3.46%
The home mortgage firm drops 10% in January and interest soars to 3.46% The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella
The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella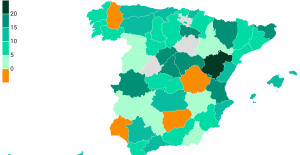 Rental prices grow by 7.3% in February: where does it go up and where does it go down?
Rental prices grow by 7.3% in February: where does it go up and where does it go down? Even on a mission for NATO, the Charles-de-Gaulle remains under French control, Lecornu responds to Mélenchon
Even on a mission for NATO, the Charles-de-Gaulle remains under French control, Lecornu responds to Mélenchon “Deadly Europe”, “economic decline”, immigration… What to remember from Emmanuel Macron’s speech at the Sorbonne
“Deadly Europe”, “economic decline”, immigration… What to remember from Emmanuel Macron’s speech at the Sorbonne Sale of Biogaran: The Republicans write to Emmanuel Macron
Sale of Biogaran: The Republicans write to Emmanuel Macron Europeans: “All those who claim that we don’t need Europe are liars”, criticizes Bayrou
Europeans: “All those who claim that we don’t need Europe are liars”, criticizes Bayrou These French cities that will boycott the World Cup in Qatar
These French cities that will boycott the World Cup in Qatar Archery: everything you need to know about the sport
Archery: everything you need to know about the sport Handball: “We collapsed”, regrets Nikola Karabatic after PSG-Barcelona
Handball: “We collapsed”, regrets Nikola Karabatic after PSG-Barcelona Tennis: smash, drop shot, slide... Nadal's best points for his return to Madrid (video)
Tennis: smash, drop shot, slide... Nadal's best points for his return to Madrid (video) Pro D2: Biarritz wins a significant success in Agen and takes another step towards maintaining
Pro D2: Biarritz wins a significant success in Agen and takes another step towards maintaining
a number of different media have in recent times drawn attention to glaring deficiencies in the management of patients who suffer from addiction and at the same time have other psychiatric problems. ”Mission audit” report in the SVT Sannes suffering and nätmediet KIT's depiction of Isaac's death in an overdose, are two significant examples of how, unfortunately, it can look like in Sweden today.
As beroendeläkare we see far too often, severely ill patients being shifted around between different healthcare providers and samhällsinstanser without anyone taking an overall behandlingsansvar. Even for those of us working in health care, it may be unclear who actually has responsibility for what – how hard is it not for the desperate patients and family?
However, a prerequisite for developing good quality health care where people do not ”fall between the cracks” is that there is a clear framework for who should do what. So, unfortunately, it is not in the day, when the responsibility for beroendevården is divided between the health services and social services.
We can't keep a system where health care denies people the psychiatric help if they use drugs, and categorically refers them to an often nonplussed social services that do not have this expertise.
The solid Missbruksutredningen (SOU 2011:35) stated in 2011 that this fundamental ambiguity leads to major practical problems. No other comparable countries organize their dependency care in this way. The investigation therefore concluded that the system should be reformed so that the responsibility for treatment is transferred to the health services. The proposal has unfortunately not been translated into reality, but in our opinion the arguments for such a reform can only become stronger in recent years.
might be able today can be diagnosed and treated with both medication and psychological approaches, just like other psychiatric diseases. Some patients also need help with such as housing, employment and the economy, and it is, of course, the social efforts is extremely important. But when it comes to diagnostics and specific treatment, there is no reason to give better treatment to patients with addictive disorders in relation to other patient groups. For other ailments, it is a matter of course that these efforts will be administered by certified staff within the health and care system, in accordance with science and proven experience. So it is not for the majority of beroendepatienter.
, namely to see addiction as a health issue, a complex disease, among others, where the individual's beteendeval plays an important role. Studies have also shown that an overwhelming majority of the population would rather seek medical care than social services for dependency problems.
New Swedish research suggests that primary care can make a big positive difference for many beroendepatienter, while more complex cases can be referred to the specialized dependency care. This means that the healthcare industry has greater opportunities to reach patients early and prevent complications.
the Knowledge of how best to help beroendepatienter with psychiatric co-morbidities has increased in recent years. A gratifying development is also that the addition of specific training in addiction for both physicians and psychologists. But the health system must be changed, so that it becomes obvious that beroendepatienter have the right to meet with staff who are trained in this type of diagnosis and treatment.
We can't still have a system where health care denies people the psychiatric help if they use drugs, and categorically refers them to an often nonplussed social services that do not have this expertise. Clinically important examples are patients with addiction, activity and attention (adhd), post-traumatic stress syndrome or bipolar affective disorder. In all these cases, there is effective treatment to offer, which also leads to substansbruket decreases. If such treatment does not come about, however, it is common to beroendeproblemen worsen, increasing the risk of long-term complications, overdose and suicide.
It is equally important to pay attention to physical comorbidity of beroendepatienter, which of course requires medical expertise. A current example is the new, highly efficient drugs against hepatitis C, which means that we within a few years, basically would be able to eliminate the spread of infections among people who inject drugs, if only we had a health care that reached and was able to help these patients over the entire country.
How to become a good a whole is up to each sjukvårdsregion and the municipality to try to resolve locally through so-called agreements. Since we have 290 municipalities in the country, it goes without saying that the system becomes unwieldy. It will also be brittle, since the small municipal units hardly have the resources to maintain a wide and competent range of medical care.
In times of strained municipal economy tends also to reduce the resources available for helping people with addiction, a group that lacks a strong voice in the public sphere and may find it difficult to defend their own rights.
An objection to changing the system is that such a reform in itself requires energy and resources, which could instead be needed in the healthcare system. Initially, it may also be practical difficulties in the transition. This is, however, short-term problems, which can largely be prevented by adequate planning and resource allocation in omställningsfasen. Therefore, they should not prevent us from creating an effective and sustainable structure for beroendevården as a whole. Fortunately, there is now a proposal from the committee on health and welfare that the government should revisit these basic questions of liability. The question is not settled, but hopefully this can lead to a very welcome change of beroendevårdens structure.
the Social services can then focus on their core functions, to assist the most socially vulnerable patients with the action that creates good conditions for the specific treatment, mainly housing and employment. Such a reform would provide the basis for a more knowledge-based dependency care, where more people would feel welcome.