 Hamas-Israel war: US begins construction of pier in Gaza
Hamas-Israel war: US begins construction of pier in Gaza Israel prepares to attack Rafah
Israel prepares to attack Rafah Indifference in European capitals, after Emmanuel Macron's speech at the Sorbonne
Indifference in European capitals, after Emmanuel Macron's speech at the Sorbonne Spain: what is Manos Limpias, the pseudo-union which denounced the wife of Pedro Sánchez?
Spain: what is Manos Limpias, the pseudo-union which denounced the wife of Pedro Sánchez?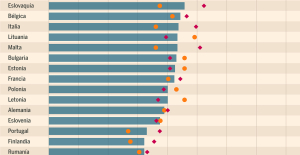 Spain is the country in the European Union with the most overqualified workers for their jobs
Spain is the country in the European Union with the most overqualified workers for their jobs Parvovirus alert, the “fifth disease” of children which has already caused the death of five babies in 2024
Parvovirus alert, the “fifth disease” of children which has already caused the death of five babies in 2024 Colorectal cancer: what to watch out for in those under 50
Colorectal cancer: what to watch out for in those under 50 H5N1 virus: traces detected in pasteurized milk in the United States
H5N1 virus: traces detected in pasteurized milk in the United States Private clinics announce a strike with “total suspension” of their activities, including emergencies, from June 3 to 5
Private clinics announce a strike with “total suspension” of their activities, including emergencies, from June 3 to 5 The Lagardère group wants to accentuate “synergies” with Vivendi, its new owner
The Lagardère group wants to accentuate “synergies” with Vivendi, its new owner The iconic tennis video game “Top Spin” returns after 13 years of absence
The iconic tennis video game “Top Spin” returns after 13 years of absence Three Stellantis automobile factories shut down due to supplier strike
Three Stellantis automobile factories shut down due to supplier strike A pre-Roman necropolis discovered in Italy during archaeological excavations
A pre-Roman necropolis discovered in Italy during archaeological excavations Searches in Guadeloupe for an investigation into the memorial dedicated to the history of slavery
Searches in Guadeloupe for an investigation into the memorial dedicated to the history of slavery Aya Nakamura in Olympic form a few hours before the Flames ceremony
Aya Nakamura in Olympic form a few hours before the Flames ceremony Psychiatrist Raphaël Gaillard elected to the French Academy
Psychiatrist Raphaël Gaillard elected to the French Academy Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV
Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV Tesla launches a new Model Y with 600 km of autonomy at a "more accessible price"
Tesla launches a new Model Y with 600 km of autonomy at a "more accessible price" The 10 best-selling cars in March 2024 in Spain: sales fall due to Easter
The 10 best-selling cars in March 2024 in Spain: sales fall due to Easter A private jet company buys more than 100 flying cars
A private jet company buys more than 100 flying cars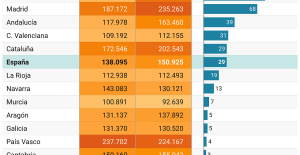 This is how housing prices have changed in Spain in the last decade
This is how housing prices have changed in Spain in the last decade The home mortgage firm drops 10% in January and interest soars to 3.46%
The home mortgage firm drops 10% in January and interest soars to 3.46% The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella
The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella Rental prices grow by 7.3% in February: where does it go up and where does it go down?
Rental prices grow by 7.3% in February: where does it go up and where does it go down? “Deadly Europe”, “economic decline”, immigration… What to remember from Emmanuel Macron’s speech at the Sorbonne
“Deadly Europe”, “economic decline”, immigration… What to remember from Emmanuel Macron’s speech at the Sorbonne Sale of Biogaran: The Republicans write to Emmanuel Macron
Sale of Biogaran: The Republicans write to Emmanuel Macron Europeans: “All those who claim that we don’t need Europe are liars”, criticizes Bayrou
Europeans: “All those who claim that we don’t need Europe are liars”, criticizes Bayrou With the promise of a “real burst of authority”, Gabriel Attal provokes the ire of the opposition
With the promise of a “real burst of authority”, Gabriel Attal provokes the ire of the opposition These French cities that will boycott the World Cup in Qatar
These French cities that will boycott the World Cup in Qatar Judo: Blandine Pont European vice-champion
Judo: Blandine Pont European vice-champion Swimming: World Anti-Doping Agency appoints independent prosecutor in Chinese doping case
Swimming: World Anti-Doping Agency appoints independent prosecutor in Chinese doping case Water polo: everything you need to know about this sport
Water polo: everything you need to know about this sport Judo: Cédric Revol on the 3rd step of the European podium
Judo: Cédric Revol on the 3rd step of the European podium
"It's a revolution," says Health Minister Karl Lauterbach. That may sound loud-mouthed, but it should get to the heart of the matter. Experts and politicians have been fighting for this draft of a reform in the German healthcare system for at least three decades, and they all had the same thing in mind: the hospitals, what they cost, what they provide, and that it is becoming increasingly difficult to bring the two into a reasonable relationship.
Now the health insurance companies have a deficit of at least 17 billion euros compared to health care that is not worth the money. It's better, it's cheaper. Lauterbach's reform addresses the greatest evil: there are too many clinics, too many operations and too many empty beds. Compared to neighboring EU countries, Germany has a record number of hospital beds per capita - and analogous to this, an exorbitant number of overnight stays, very often without a valid reason. "Organized deprivation of liberty," etches a health expert.
Reinhard Busse, Professor of Health Care Management at the TU Berlin and member of the expert commission that has now presented the draft for the hospital reform, puts it succinctly: "On average, we treat patients twice as often as inpatients than our European neighbors." That has to be not be, puts a strain on patients and health insurance companies, but brings money into the hospital coffers.
At its core, the reform concept of the commission, which Lauterbach wants to reformulate into a law, consists of a single sentence: We need far fewer but much better equipped hospitals. One in three of the almost 2,000 German hospitals doesn't even want to be called a "hospital" by Busse: "These are just buildings with beds."
In Denmark, the problem is only too well known – with hindsight. The Danes have succeeded in an exemplary hospital reform, small clinics closed down, the best specialist doctors concentrated on the large ones in developed, modernized and first-class equipped care centers. There are almost as many nursing staff available for each bed in a normal ward as in a German intensive care unit. Which does not mean that the Danes have more nursing staff. It's just fewer beds.
Busse therefore sees only one solution for the German health disease: "There must be fewer hospitals so that we have more staff per hospital and per bed".
In addition to health economist Busse, two other members pushed ahead with the draft reform on behalf of the federal government: health economist Boris Augurzky and intensive care physician Christian Karagiannidis. Her proposal envisages three types of hospitals: primary care for common surgical procedures and emergencies. You bill per day (i.e. without accommodation costs) instead of per treated case (with any length of stay). Secondly, the standard and priority providers for patients who are not in the best of hands with the primary providers.
Third, the maximum providers. The best that can be had in terms of specialists and medical equipment is offered here. There should be a “retention fee” for this effort, regardless of the number of cases.
A small, non-representative survey by WELT among health insurance experts, medical economists, politicians and hospital managers revealed that the chances of reform are only between 40 and 60 percent. From a technical and factual point of view, there is hardly anything to shake up on the plan. But politically yes, because the reform has to pass through a trellis of well-armed lobbyists and association representatives.
Above all, local and state politicians could get in the way. Because the fate of the hospitals is in the hands of the federal states, the district administrators who are attached to their local hospital, the prime ministers and the health ministers of the states. Almost everyone fights for the preservation of even the smallest hospitals.
Lauterbach knows the game. Now he has to organize majorities and allies. However, the example of the most important like-minded person and comrade-in-arms for the reform, NRW Minister of Health Karl-Josef Laumann (CDU), gives an idea that this could go wrong.
Laumann is much further ahead in implementing the reform than the Federal Minister of Health. The "big operation", as Laumann calls the restructuring of the hospital landscape in North Rhine-Westphalia, has been in full swing since September. In order to end the "ruinous competition" between the clinics, Laumann pushed for specialization. 337 general hospitals are to be transformed into heart, joint or cancer clinics, some are to be merged, others closed.
In addition, the rule of thumb should apply: basic care for internal medicine, surgery and intensive care must be accessible from any point in North Rhine-Westphalia within 20 minutes. It's anything but a "hospital closure plan," says Laumann. Exemplary North Rhine-Westphalia, it should say in the Federal Ministry of Health.
Although they agreed on the matter, Lauterbach drove his ally into the parade. Laumann, so Lauterbach spread in his constituency (Leverkusen/Cologne-Mülheim), was about to close the largest local hospital. Laumann immediately denied it.
Two days ago, during the conference of state health ministers, Laumann was to be found in the camp of those who were more critical of reform: "It must be crystal clear: the states are responsible for hospital planning, and it must remain so."