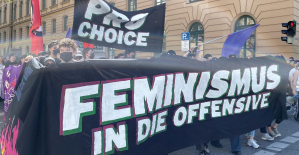
 Germany: abortions should be authorized up to 12 weeks, concludes a commission launched by Olaf Scholz
Germany: abortions should be authorized up to 12 weeks, concludes a commission launched by Olaf Scholz Knife attack in Australia: who are the two French heroes congratulated by Macron?
Knife attack in Australia: who are the two French heroes congratulated by Macron? Faced with an anxious Chinese student, Olaf Scholz assures that not everyone smokes cannabis in Germany
Faced with an anxious Chinese student, Olaf Scholz assures that not everyone smokes cannabis in Germany In the Solomon Islands, legislative elections crucial for security in the Pacific
In the Solomon Islands, legislative elections crucial for security in the Pacific Covid-19: everything you need to know about the new vaccination campaign which is starting
Covid-19: everything you need to know about the new vaccination campaign which is starting The best laptops of the moment boast artificial intelligence
The best laptops of the moment boast artificial intelligence Amazon invests 700 million in robotizing its warehouses in Europe
Amazon invests 700 million in robotizing its warehouses in Europe Inflation rises to 3.2% in March due to gasoline and electricity bills
Inflation rises to 3.2% in March due to gasoline and electricity bills Against drug trafficking, the mayor of Amsterdam advocates the regulation of cocaine
Against drug trafficking, the mayor of Amsterdam advocates the regulation of cocaine Hachette Livre removes Isabelle Saporta from management of Fayard
Hachette Livre removes Isabelle Saporta from management of Fayard Where is the MSC Aries, the ship boarded by Iran?
Where is the MSC Aries, the ship boarded by Iran? Denis Olivennes at Le Figaro: “CMI France discusses with Natacha Polony the future of Marianne”
Denis Olivennes at Le Figaro: “CMI France discusses with Natacha Polony the future of Marianne” 2024 Candidates Chess Tournament: Relive the Crucial Nepo-Gukesh Game
2024 Candidates Chess Tournament: Relive the Crucial Nepo-Gukesh Game Borgo, by Stéphane Demoustier: locked outside
Borgo, by Stéphane Demoustier: locked outside Release of hostages and immediate ceasefire: at the Venice Biennale, the Israeli pavilion resonates with Gaza
Release of hostages and immediate ceasefire: at the Venice Biennale, the Israeli pavilion resonates with Gaza Two Russian artists declared “terrorists and extremists” because of a play
Two Russian artists declared “terrorists and extremists” because of a play Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV
Skoda Kodiaq 2024: a 'beast' plug-in hybrid SUV Tesla launches a new Model Y with 600 km of autonomy at a "more accessible price"
Tesla launches a new Model Y with 600 km of autonomy at a "more accessible price" The 10 best-selling cars in March 2024 in Spain: sales fall due to Easter
The 10 best-selling cars in March 2024 in Spain: sales fall due to Easter A private jet company buys more than 100 flying cars
A private jet company buys more than 100 flying cars This is how housing prices have changed in Spain in the last decade
This is how housing prices have changed in Spain in the last decade The home mortgage firm drops 10% in January and interest soars to 3.46%
The home mortgage firm drops 10% in January and interest soars to 3.46% The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella
The jewel of the Rocío de Nagüeles urbanization: a dream villa in Marbella Rental prices grow by 7.3% in February: where does it go up and where does it go down?
Rental prices grow by 7.3% in February: where does it go up and where does it go down? Europeans: the schedule of debates to follow between now and June 9
Europeans: the schedule of debates to follow between now and June 9 Europeans: “In France, there is a left and there is a right,” assures Bellamy
Europeans: “In France, there is a left and there is a right,” assures Bellamy During the night of the economy, the right points out the budgetary flaws of the macronie
During the night of the economy, the right points out the budgetary flaws of the macronie Europeans: Glucksmann denounces “Emmanuel Macron’s failure” in the face of Bardella’s success
Europeans: Glucksmann denounces “Emmanuel Macron’s failure” in the face of Bardella’s success These French cities that will boycott the World Cup in Qatar
These French cities that will boycott the World Cup in Qatar Bundesliga: Naby Keita suspended by Werder Bremen until the end of the season
Bundesliga: Naby Keita suspended by Werder Bremen until the end of the season Euro 2024: the Blues reveal their opponents for friendlies in June
Euro 2024: the Blues reveal their opponents for friendlies in June Cycling: De Marchi wins the 2nd stage of the Tour of the Alps
Cycling: De Marchi wins the 2nd stage of the Tour of the Alps Paris Olympics 2024: Joris Daudet (BMX) candidate to be French flag bearer
Paris Olympics 2024: Joris Daudet (BMX) candidate to be French flag bearer
In a reply to our article on tillgänglighetsproblemet in the Swedish health care has Fredrik Lennartsson formulated SALAR's views on the matter. In many respects, shared our view, but in the crucial question of the role of principals expressed not unexpectedly dissent
According to Fredrik Lennartsson has long waiting lists have been a ”high-priority issue in many years”. The outcome has become a duplicate queue during the last few years. Despite the different perceptions about the underlying problems, we seem to be, however, agreed that the current sjukvårdsapparat not able to handle the need.
It is about the effective provision of skills, digitisation and conversion to a close and the care. The regions ' work in these areas has so far not been successful. Despite the fact that the SKL announced two years ago to 1 January 2019 would be independent of the hyrpersonal increase the use of agency staff and the cost for the year 2018 is expected to exceed the five billion became the bill of 2017.
In the ongoing procurement of a ”future vårdinformationssystem” will the regions to land not in a system but two or maybe three. Sweden has, compared to several other countries, an underdeveloped near care including long-term shortage of doctors. It's hard to believe that the future with the current principals will be better. The problem with the lack of availability is, in essence, a system failure.
In our proposal for a more efficient care and included several parts.
the Order/assignment and follow-up of outcomes requires knowledge of the sjukdomspanorama and vårdkonsumtionsmönster, the skills to evaluate the medical development and the ability to assess the costs for the rendered vårdprestationer. The reasonableness of the parallel handle this within the 21 regions is not difficult to question.
basically, this is a question of fairness. Sjukvårdslagens requirements on the care on equal conditions can not be met by the regions and municipalities, with a diversity in population structure and the tax base. Different equalisation system is a blunt instrument in this regard and reports on the villkorsskillnader between different regions daily. A week was alerted to the example of unequal therefore.
A state beställarfunktion shall formulate contracts, establish what that shall be done.
the Regions shall, with his knowledge of the local circumstances in which providers address the issue of how this is to be enforced.
unfortunately, It is not as Lennartsson argues that ”the systematic and long-term local work with close knowledge of the local and regional needs” resulted in good availability. On the contrary, this system resulted in the current kösituationen.
We maintain that the changes required to manage the health care access problems will not be able to be implemented without the state is made to the client and to the funder of all samhällsfinansierad care.


















